We had so much fun becoming a family of 5 over the summer. Besides being slow to gain weight, Ivy was doing well. She was so tiny and snuggly and I loved every minute of being her mom! Excuse me while I add too many pictures before I keep going with the story…

Forever Home Run! 
Great Papa! 
How many of us fit on my bed? 
Just a chat with Gaga 
Aunt Lauren 
Naps with Poppy are the best! 
Mommy & Daughters Date 
He loves snuggling his sister! 
Unicorn Hat 
Incredible Ivy 
Could she be any cuter? 
All bundled up at the pumpkin patch 
Apple Orchard Trip 
Baby wearing at the farm 
Halloween – The Incredibles! 
The Sweetest Siblings!
In September, several things seemed to happen at one. First, we noticed that Ivy would get very upset whenever she was laid on her back or in the car seat. She had always spit up quite a bit, but that in conjunction with the unhappiness on her back, led us to ask the pediatrician about reflux. She agreed that Ivy seemed to show signs of reflux, and combined with her poor weight gain, we decided to try medication. She started Ivy on Zantac. This medicine was given orally, but caused Ivy to splutter and choke every time we gave it to her. Around the same time, her nursing started to change. She always had been nursing for only about 5 minutes before getting tired, every 90-120 minutes. All of the sudden, this jumped to nursing for 1-2 minutes every 30-90 minutes. AROUND THE CLOCK. We also started trying to give Ivy a bottle because she would need to take one when I went back to work in mid October. We tried everything we could think of, but she just could NOT figure it out. She wasn’t refusing to take it, she would take the nipple in her mouth, but just seemed totally unaware of how to suck!
So the combination of all these things led us to a conversation with her Neuro-Developmental Pediatrician about feeding. She said that around 3 months, babies start to lose the reflex to suck. When infants have really troublesome acid reflux, they learn quickly that eating is painful and so they stop doing it. She said it sounded like Ivy was nursing just enough to satiate her initial hunger and then stopping. She sent us to feeding therapy and we had the first discussion about a possible G-tube.

So tired from eating! 
Physical Therapy 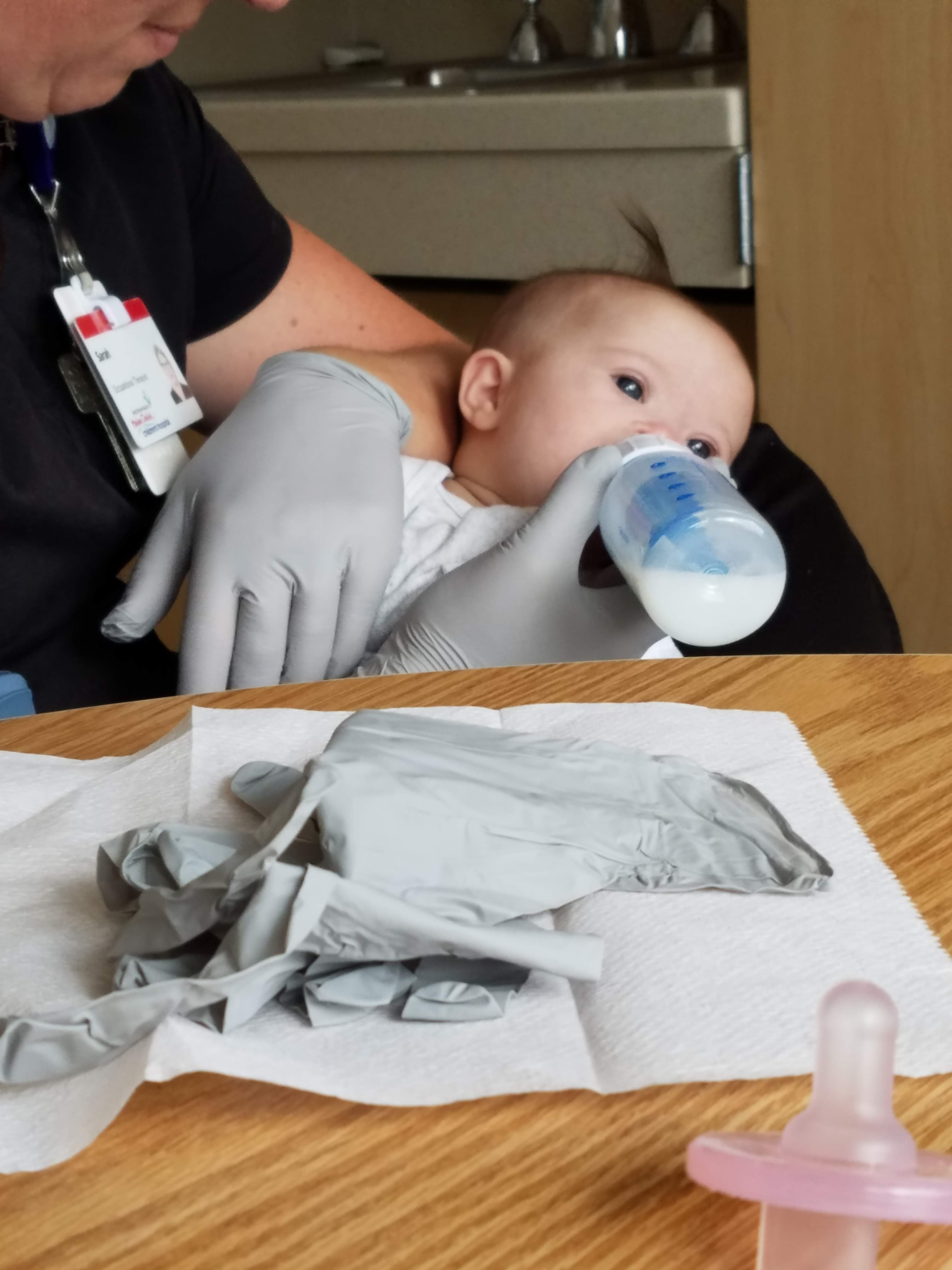
Feeding Therapy
We started feeding therapy with very little success. Ivy was not getting the hang of sucking from a bottle or a pacifier. She had a very strong gag reflex and would gag every time a finger, bottle, or pacifier was put in her mouth. Between the choking on medicine, and the struggles with the bottle, the feeding therapist decided we should have a swallow study done. A swallow study is performed under live x-ray so that a speech therapist can see whether a person is aspirating (taking liquid into their lungs) while drinking. Ivy’s swallow study was a bit more complicated because generally a bottle of milk mixed with barium (so that it shows up on the x-ray) is given to watch swallowing, but Ivy could not take a bottle. The therapist ended up using a syringe to give Ivy little amounts of the milk/barium mixture. After each small amount of milk was syringed in, we watched on the live x-ray as Ivy attempted to swallow it. It became immediately apparent that Ivy was working SO hard to swallow. Her muscles seemed very disorganized and it would take her seven to eight swallows to get just a couple milliliters of milk into her tummy. We were able to confirm that she was not fully aspirating, but there were several instances where liquid would penetrate her airway but she would be able to work it back out. Most likely, a feeding tube would be in our future.

Then Ivy got sick. In an effort to ensure she did not have aspiration pneumonia, the doctor ordered a chest x-ray. It was a Friday afternoon and the doctor called with the results. It was not our normal pediatrician. She immediately told me that the x-ray was negative for pneumonia but it did find a diaphragmatic hernia. Then she said, “Don’t Google it, we’ll get in touch with you next week.” So naturally, I panicked! One of my new Ds mom friends was also a NICU nurse, so I immediately texted her. She said the reason the doctor told me not to Google it was that there are two types of diaphragmatic hernias. A hernia is a weakness or hole that should not exist in the middle of a muscle which allows organs or tissues to push through. The most common kind is caught during pregnancy occurs in the side and back of the diaphragm and involves a large portion of the abdominal organs up into the chest cavity, which impedes lung growth, and requires surgery immediately after birth. Ivy had the much more rare kind called a Morgagni diaphragmatic hernia which occurs in the front of the diaphragm so that only a portion of her intestines was protruding into her chest. It had not significantly impeded her lung growth which is why we didn’t know about it. Most likely, it was causing some of her reflux issues, and so it would need to be repaired.

Sick little girl! 
Example of a Morgagni Diaphragmatic Hernia X-Ray
Our next step was to meet with the pediatric surgeon to discuss tube placement and hernia repair. He told us that he could do both during the same surgery, which was such a relief! Unfortunately, he told us that the anesthesiologists will not put a baby under anesthesia if they have recently been sick with an upper respiratory infection, which Ivy had just had. He said we would need to schedule it out 6 weeks. The big problem with that was that I was supposed to start teaching again because I had used all of my sick days for maternity leave. I couldn’t go back to teaching until she had a tube because she was not able to eat enough orally without me. As a teacher on maternity leave, I’m only paid for the sick days that I have accrued. Any extra days I took would be unpaid which cost a significant amount of money that we couldn’t afford to lose. He suggested that we have a tube placed through her nose to get us to the surgery date. So a few days later, Ivy and I traveled to Helen DeVos Children’s Hospital (which is luckily only 10 minutes away for us) for an overnight stay to get her nasal tube placed as well as some testing done.
There are two types of nasal feeding tube. A Nasal Gastric (NG) Tube goes through the nose, down through the esophagus, and into the stomach. A Nasal Jejunum (NJ) Tube goes through the nose, down through the esophagus, bypasses the stomach, and into the small intestine. Between the neurodevelopmental pediatrician, the pediatric surgeon, and I, we decided that an NJ Tube made the most sense for Ivy because of her reflux. Any nasal tube keeps the sphincter between the esophagus and stomach open constantly which allows for acid to reflux much more easily. If we bypassed the stomach and put milk directly into her intestine, there would be a much smaller chance of increased reflux troubles.
We arrived to the hospital in the morning, and got admitted to a room. Around noon, they came up to get us for the procedure. We went down to the radiology department as the tube needs to be placed under live x-ray. Luckily some of the tests Ivy needed could be done right before the tube placement so that we didn’t have to come back twice. They strapped Ivy to a rotating board so that she was immobilized and they could rotate her body to get different views. They started with the upper GI test. During this test, they syringed a barium formula into her mouth and used the x-ray to visualize her upper gastrointestinal tract including her esophagus, stomach, and duodenum. She wasn’t able to get enough barium in by syringe so they ended up putting a tube through her nose into her stomach so that they could get enough to go through to her duodenum. Everything looked normal which was great.

Next, they did a lower GI test. Ivy stayed strapped to the table, but the put the barium solution in an enema so that they could map out her lower gastrointestinal tract. Apparently, the physicians assistant that was running the test did not know about her diaphragmatic hernia. The look on his face when the dye started going up into her chest cavity was so funny. He turned to me with wide eyes and I said, “Yup, we know part of her intestine is in her chest, don’t worry! She has a diaphragmatic hernia!” He was pretty excited to see a Morgagni Diaphragmatic Hernia for the first time in real life! Besides some redundancies in her intestines, her GI tract looked good which was great! The surgeon just wanted to make sure he didn’t need to do anything else during the surgery.
Finally, the used the live x-ray to place the NJ tube. By this time, Ivy was no longer very thrilled to be strapped to this table. Add to that the tube being forced down her nose and it was pretty tough for both of us! Using the live x-ray, the PA threaded the tube down her nose, through her esophagus, through her stomach and duodenum, and stopped at the jejunum. He then taped the tube in place while teaching me how to do it when I would have to replace the tape.

Snug as a bug in a rug 
DeVos Children’s Hospital has the best Child Life Specialists! They gave us an Elsa with an NJ tube to make it less scary for Zoe and Eli! 
Practicing tummy time at the hospital!
Once we got back to our room, the nurse hooked her tube up to a pump and added my breast milk to the pump bag. With a G tube in the stomach, you can give a ‘bolus’ feed which is several ounces at once like a ‘meal’ would be. Because the tube was going into her intestines which cannot hold that much without rupturing, she would need to be on continuous feeds. That means that for 20 hours of the day, milk would be slowly pumped into her tube and we were able to have 4 hours a day disconnected from the pump. We stayed at the hospital overnight because they started the feeds very slowly and throughout the day and night increased how much she was getting until she was at the goal of 24 milliliters per hour. Everything went smoothly, so we were discharged the next day with a whole new set of medical equipment. It was definitely a learning curve as we figured out how to attach and work the pump, carry the IV pole around the house, keep the tube out of her tiny hands, give medicine through the tube, and how much milk to put in at a time. The pump does a really fun beeping noise if something goes wrong (a sound that I’m pretty sure will haunt my dreams forever!) like a kink in the tube somewhere or if too much air gets in. We slowly learned!
At this point Ivy was finally getting all the calories she needed, so it was time for me to return to work. Because we needed to keep her away from other kids so that she would be healthy for surgery, family and friends helped us by coming to our house and watching Ivy during the work day. We were so blessed by family and friends. We had to tell Zoe and Eli that they couldn’t touch or kiss Ivy for the next several weeks which was particularly devastating to Zoe. It would all be worth it if we could make it to our surgery date which was going to be December 5th!
To be continued…



